Preschool A List of The Most Popular Preschool Supplies We all know that shopping for school supplies can be a difficult task. Now imagine prepping...
college, Education How to Establish Residency in Florida For College If you are moving to a state for college, the first thing you must do is research what is needed...
Tech What is Roblox? With approximately 37.1 million users worldwide, over the last few years Roblox has become one of...
Tech How Do Solar Panels Work on a House? As consumers become more aware of the negative environmental impacts of fossil fuels and increasingly desire energy independence, the solar...
August 10, 2016 National Youth Day National Youth Day In Albania IntroductionInternational Youth day is a..
August 10, 2016 Anniversary of the Revolution in Algeria History The French ruled Algeria for almost 132 years, they..
January 16, 2021 What Is A Starburst Galaxy? The Hubble Heritage Team, N. (1999, December 7). Starburst Galaxy NGC 3310 [Digital image]. Retrieved January 10, 2021, from For....
January 15, 2021 Coca-Cola Space Science Center About The Coca-Cola Space Science Center The Coca-Cola Space science Center (CCSSC) was established in 1996, and it is owned....
January 9, 2021 What kinds of objects lie in the disk of our galaxy? Once we are allowed to examine the Galaxy to which we reside, we often find ourselves awe-stricken by the immense....
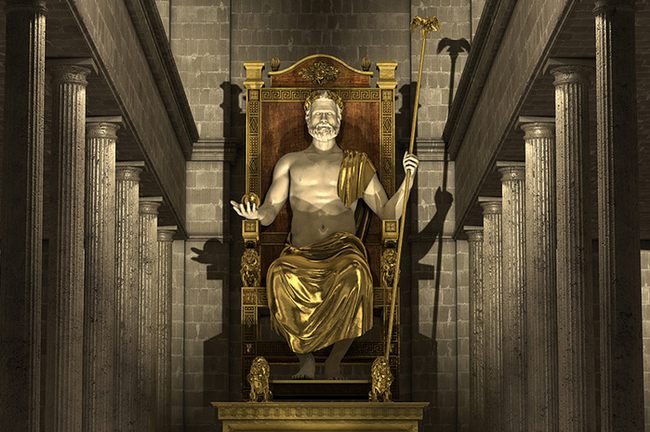
July 29, 2017 The Statue of Zeus at Olympia is considered a part of the collection for the Seven Wonders...
July 29, 2017 What is the Temple of Artemis at Ephesus? The Temple of Artemis at Ephesus is a part...
July 29, 2017 The Colosseum is a famous amphitheater that resides directly in the heart of Rome, Italy. It is...
July 29, 2017 What is the Mausoleum at Halicarnassus? The Mausoleum of Halicarnassus was a structure designed by Pythius of...
January 17, 2021 Change The Snooze Time on an iPhone Many of us rely on an alarm to wake us up in the morning, and so many of us own iPhones.
January 16, 2021 How to turn off wifi calling What is WiFi calling? Wi-Fi calling is a service for Android and iOS smartphones. This service provides the owner with the
January 15, 2021 How To Create a PST File What is a pst file and How To Create a PST File Microsoft Outlook stores its emails and other items in